Susan Leigh Deppe, MD, offered a popular two-part session at IIRP's 16th World Conference on emotion, affect theory and restorative practices. The piece below describes some of the main points of her presentation.
SO THAT’S WHAT’S GOING ON!
UNDERSTANDING EMOTION IN RESTORATIVE PRACTICES
Communities and schools struggle with behaviors such as crime, bullying, rudeness, and violence. These echo popular culture, where people often act macho and explosive. Actions and attitudes are absorbed out of awareness from the emotional milieu surrounding us, whether family, media, faith community, or schools. Our emotional patterns are sculpted by life experience. People who manage emotion poorly are more likely to be alienated from others or involved in substance abuse, crime and other negative behaviors.
No one should expect schools or towns to repair damage caused by severe neglect, trauma, or mental illness. But we all are affected by those factors, and there are things we can do. The more time we spend with people, the more impact we can have on them. We can teach people explicitly about their emotions, and if we immerse people in a healthy emotional climate, they can develop better emotional patterns. There are two pieces: Explicit education about emotion, and restorative practices. Let’s look at them.
The affect and script paradigm of Silvan S. Tomkins, PhD, and Donald L. Nathanson, MD, is a powerful tool to understand emotion and help people heal and grow. It helps us view people in the context of biology, biography, family, and culture, and explains why restorative practices work. There are nine innate affects (biological emotion programs), each with a characteristic trigger, feeling, and facial expression. Two affects feel good, the range from interest to excitement and from enjoyment to joy. Surprise-startle interrupts us and resets the system. Six negative affects feel bad in different ways: Anger-rage, fear-terror, distress-anguish, dissmell (“Ewwww!” the root of contempt), disgust, and shame-humiliation. Innate shame occurs when there is an impediment (slowing or partial stop) to the expression of one of the two positive affects, as there often is when we experience failure, rejection, hurt feelings, or embarrassment, or when someone does not resonate with our enthusiasm. The affects are amplifiers that make things feel good or bad and motivate us. We define emotion as feeling an affect, plus memory of prior experience of that affect. Innate affects link with life experience to form scripts, powerful emotional rules, of which we are usually unaware. Most of adult life is managed by scripts. We are wired to want to express and maximize positive affect, express and reduce negative, and get affects out on the table. Personality is the general pattern of scripts used by a person. Scripts may be adaptive or maladaptive. Humans are complex. Tomkins’s paradigm has enormous power to explain what we see. We can study the language of emotion, personality development, different intensities of affect, affect modulation, emotional contagion, script change, empathy, intimacy, and community. We can explore how factors such as illness, fatigue, or drugs change the affect system, and some of the reasons why people engage in substance abuse and other risky behaviors. Adults and kids can learn to observe affects and scripts in themselves and others.
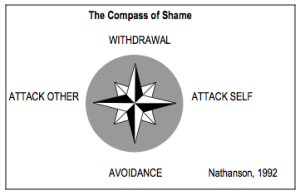
Nathanson points out that people in Western societies are handling the shame family of emotions differently now than in the past. In the early twentieth century, people tended to go to withdrawal and attack self (deference). There was much more stigma attached to being seen as shamed in the eyes of one’s neighbors. Now people are more likely to act out in the avoidance and attack other poles. This is a dangerous change. Substance abuse raises the risk of violence, due to impulsiveness or increased anger, for example.
The healthy response to shame, of course, is to tolerate its discomfort, soothe myself, acknowledge any responsibility I might have for hurtful or inappropriate behavior, remind myself that I am still a good person, and learn from the experience. However, that mature response is not easy! Learning it requires a supportive environment and a lot of practice.
We only change when it is safe to look at what shame affect is telling us. Emotionally safe environments are loving and supportive, call us on our behavior when we are out of line, push us to be our best, give positive feedback, respect us, and require us to respect others. Many families, schools, and faith communities provide these conditions, of course. How can we make them available for everybody, so we can all learn and practice healthier emotional skills? A whole school (or whole community) restorative approach does exactly that!
Restorative practices work because they are based on how we are wired: We want to share and increase positive affects, share and reduce negative affects, and remove impediments to affect expression. Restorative or affective questions allow people to tell their stories, express underlying affect, and practice empathy. In a restorative process, participants typically move through more distancing and toxic emotions (rage, fear and dissmell) first, then surprise, distress, and shame. Any participant may feel shame. Shame is only triggered when there is a positive bond, and signals openness to healing or repair. Marie Fitzgerald talks of a shift into “collective vulnerability.” Participants begin to feel the need to make it right with each other. Finally, they move into the positive affects of interest and joy as they agree on how to make things right. Rituals and agreements reinforce new patterns of actions and affects.
Some programs for bullying, anger, drugs, etc., do not work because they are treating symptoms. Underlying many problems is the inability to manage emotion. Cognitive “education” alone does little to change the largely unconscious but powerful scripts by which we function. To shift these powerful emotional rules requires intense affective experience. We can teach people about healthy emotion, but they really have to live it — over and over. For that reason, restorative practices are most powerful when used as a way of life, not an occasional intervention. The younger we start the better. ”Band-Aid” solutions will not reverse the cultural shift toward avoidance and attack other shame scripts. The answer is prevention: Explicit affect education and long-term immersion in a restorative milieu. It is a highly ethical, scientifically-based “vaccine” against violence and conflict. Benefits include big drops in problem behaviors, crime, and conflict, and better school and community cultures. Healthier, more resilient kids become healthier adults.
Susan Leigh Deppe, MD, is a Clinical Assistant Professor of Psychiatry at the University of Vermont College of Medicine and is on the Board of Directors and Faculty of The Tomkins Institute: Applied Studies in Motivation, Emotion, and Cognition. In addition to private psychiatric practice, she applies Tomkins’s work to spirituality, restorative practices, ideology and political behavior.
The Tomkins Institute offers study groups, conferences, online resources, and a lively and varied community of people with whom to share learning and positive affect. www.tomkins.org. Twitter: @TomkinsInst
Copyright 2013 by Susan Leigh Deppe, M.D. Much of this material is from the lectures of Donald L Nathanson, MD, and Vernon C. Kelly, Jr., MD, and is used by permission. Acknowledgment is also made to the IIRP.